Diabetic macular edema (DME) is one of the main causes of poor vision in diabetic patients. As the number of patients with diabetes mellitus is projected to increase exponentially worldwide, the incidence of DME is also expected to rise. This condition is characterized by the accumulation of fluids and thickening of the macula, the region in our eye which is most important for our central vision. The fluids are a result of leaky blood vessels damaged by the effects of diabetes. DME can occur by itself or simultaneously with diabetic retinopathy (DR), another visually-threatening eye condition from complications of diabetes mellitus.
Risk Factors
Duration of diabetes, poor glycemic control, hypertension, and renal impairment are among the risk factors for the development of DME. Thus, it is important to get your eyes checked when you have been diagnosed with diabetes mellitus, and to make sure that all other concurrent systemic illnesses are managed optimally.
Symptoms
Because the earliest stages of DME are usually asymptomatic, many diabetic patients are often unaware they have developed such complications. The symptoms are somewhat dependent on the location of the edema within the macula. If the edema occurs outside the centre of the macula (non-centre-involved DME), patients may not notice any change in their vision. However, if the edema occurs or spreads to the central macula, patients generally experience progressive vision loss that occurs anywhere from weeks to months after the initial symptom.
Tests
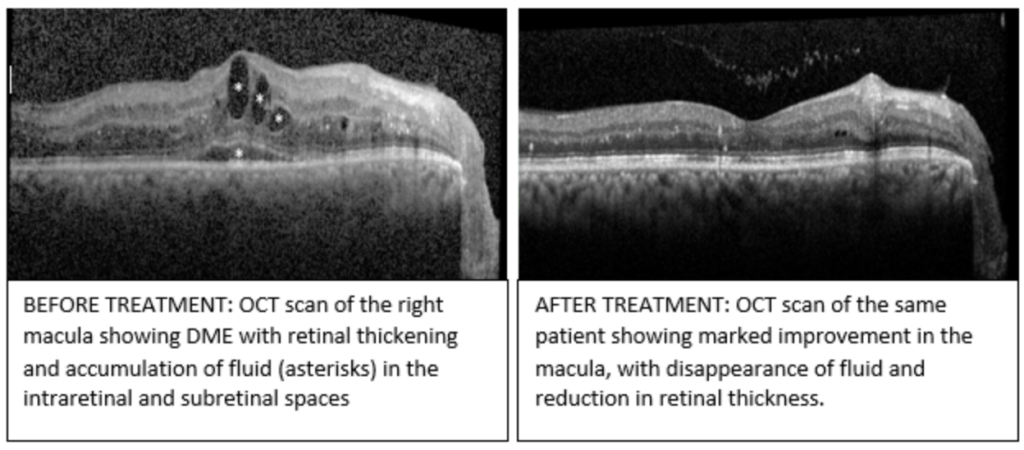
A comprehensive eye examination should include checking of visual acuity (for both distance and near), intraocular pressure measurement, and a dilated eye examination. An optical coherence tomography (or OCT in short) is now routinely performed to quantitatively measure the central macular thickness as well as to qualitatively assess the changes in the microstructures of the macula. The OCT scans are usually repeated from time to time to monitor the condition as well as to gauge treatment response.
Treatment
The need for DME treatment depends on the severity as well as the location of the edema. Select cases may be managed conservatively with careful monitoring over a series of follow-up visits. More severe DME that is visually-threatening need early treatment. Traditionally, slit-lamp laser therapy was the gold standard for treatment of DME. However, it has now been largely replaced by intravitreal injection of anti-vascular endothelial growth factor (anti-VEGF) agents. If your doctor has advised for anti-VEGF injections, do bear in mind that treatment is usually over a prolonged period of time to achieve optimal results. The injections are usually initiated monthly for the first 3 months (loading phase), followed by further injections (maintenance phase) depending on the improvement seen. However, in contrast to intravitreal anti-VEGF injections in other eye conditions such as age-related macular degeneration (AMD), studies have shown that the number of injections needed gradually decreases after the first year. It is also especially important to optimize the other systemic co-morbidities to ensure the best outcome of your DME treatment.